By Kate Ryder, Founder and CEO, Maven
With a $45m Series C round, one of the largest ever by a female founder in women’s and family health, Maven is positioned to make durable change for patients and payors alike. We also know that quick fixes won’t work. Here’s what’s required to build a new, better system.
Working on the front-lines to improve women’s and family health, it’s easy to revert to impassioned calls for change. Gaps in care, particularly around pregnancy and starting a family, are painfully apparent, stubborn, and simply not right.
Entreaties for change have their place, and indeed are critical. But this won’t be one of them.
Rather, this is about what it takes to make durable change in a space full of buzzwords and high hopes; about executing unglamorous legwork within the constraints of the current healthcare system; and about avoiding tick-the-box traps or simplistic shortcuts that fall short of real impact.
When we founded Maven, in 2014, women’s and family health was a backwater. My team and I spent our first few years landing the notion that there was a problem: That 43% percent of new moms leaving the workforce after birth, when 75% want to stay, is bad for moms, families, and companies. That America having the highest maternal mortality rate in the developed world is unacceptable. That lagging support for the 20% of millennial couples starting LGBT+ families leaves employees frustrated and payors and companies vulnerable.
These points are now thankfully obvious throughout the healthcare industry — and initiatives to address them have even become somewhat popular. The upshot has been a lot of good intention, but sadly also a scatter-shot of solutions, many of them too superficial to make real progress against the stark underlying problems. At Maven, we don’t know all the answers, but we do know that gaps in family health won’t be fixed with a band-aid, an aggregator app, or passive content.
Maven has always had a clear north star — solving the biggest pain points for women and families — and operated with a genuine willingness to mold our business to the gaps we observe in the market. Guided by the 5 million patients we’ve helped, the 1,700 doctors and specialists in our telemedicine network, and the 100+ clients we serve, we now have a clear point of view on where care breaks down, and what meaningful, sustained change looks like for both patients and payors.
We also now have the capital to support our theses and invest in the long term. Today, we are announcing a $45m Series C — one of the largest funding rounds by a female founder/CEO in women’s health — all of which we are deploying to double-down on support for women and families.
Here is our point of view on what it takes to build a better and more modern foundation in women’s and family health.
1. Keeping tightly focused on access — the single most critical gap in care
Maven has the largest women’s and family health telehealth network in the country — and we invested in building this for a reason. Basic access is the single most critical gap we see in care. The most flagrant example is that 50% of U.S. counties don’t have an OB-GYN — but more subtly, critical specialties like lactation consultants, genetic counseling, or doula support frequently aren’t baked into reimbursement models, even where they exist.
Maven is built to ensure:
- Access to near-instant care, through whatever channel you find most useful: virtual visit, telephone, message, or in some cases, a referral in-person
- Access to high quality providers, no matter where you live
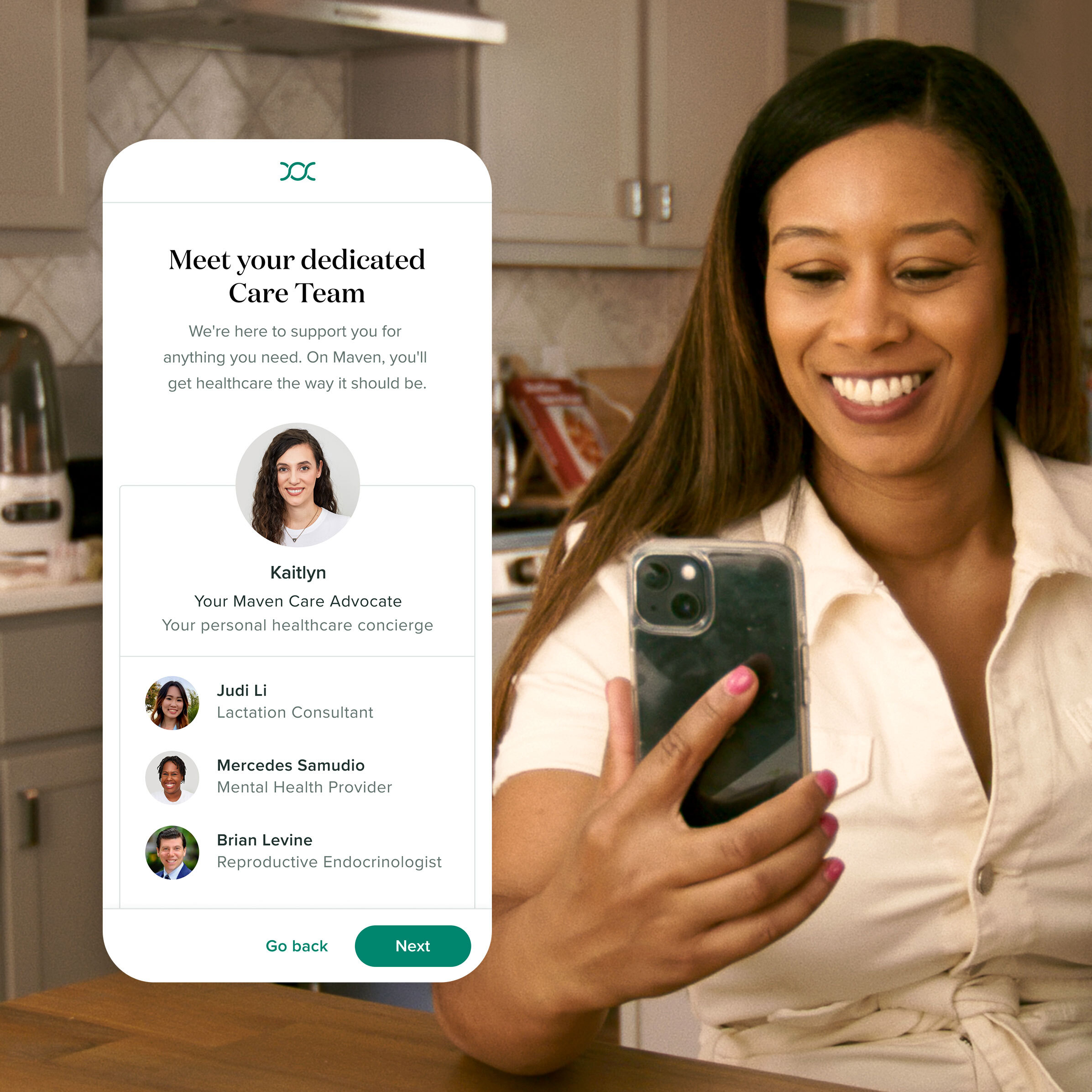
- Access to medical generalists and specialists alike — not just a doctor or nurse practitioner, but women’s health physical therapists, adoption coaches, maternal mental health providers, pediatric occupational therapists, career coaches, and a wide variety of other specialities
- Access to providers of a specific race, ethnicity, sexuality, or gender — or who speaks a specific language
- Access to support for common but frequently uncovered concerns like miscarriage, LGBT+ parenting, or single parenting
2. Doubling-down on care coordination — and ensuring that patient advocates have the deep and specific vertical expertise needed to yield results
Given the complexity of the health system, it has never been more important to have a coherent and informed understanding of options. This includes managing across a range of providers as well as navigating payments, benefits options, health plan options, and the myriad administrative burdens of starting a family. Only 9% of the general population report understanding their health benefits, and 72% of mothers report low health literacy. Many great advocacy models are emerging, but truly driving outcomes requires more than support — it requires expertise. Advocacy in women’s and family health must straddle traditional healthcare and the practical realities of working parenthood, as well as partner closely with someone’s health plan to make everything easier to navigate. More than half of our members report that our care advocates are their first call to understand benefits and coverage, which is why we staff 24/7/365. It is also why our care advocates are trained subject matter experts equipped to steer registrants without a doctor (30% of maternity patients, 45% of fertility) to an OB/GYN with WHO-standard C-section rates, or to a fertility clinic with high success and single embryo transfer rates.
3. Doing the hard but necessary work of integrating sophisticated technology with a human-centric care model, because that nexus is what drives outcomes at scale
For at least as long as Maven has existed, there has been excitement about technologies that replace patient-provider interactions in healthcare — from chatbots, to asynchronous care options, to content sites and patient-to-patient forums. Some of these technologies hold promise, but what remains clear to us is that they will supplement, not replace, one-on-one provider interactions — and that a tech-enabled human-centric model is still the key to unlocking better outcomes.
At Maven, we have found a blended model of telemedicine, care advocacy, and educational content is table stakes within digital health — and particularly so in women’s health. Anyone who suggests otherwise is not talking to postpartum moms (or can’t figure out how to build telemedicine themselves). Seventy-six percent of Maven members say the relationships they’ve built with our providers are their top source of value, and something they can’t get anywhere else. We continue to see this tech-enabled, human-centric approach as the key to driving improved outcomes in C-Section rates, reduced ER rates, and NICU admission rates. Content is a critical supplement, but trying to change behavior with content alone — when the internet is crowded with free content — is a fool’s errand. Proactive human outreach, and timely telemedicine interventions, are essential components of change.
4. Relentlessly focusing on the needs of the patient
At Maven, we stay focused on a simple formula: When patients use our product, we generate ROI for our clients. This philosophy means that we don’t take product shortcuts. We will never present quick-fix aggregator services, or direct patients to subpar products, because we know that approach will ultimately limit the impact of our product, and the value we create for clients. As a result of this approach, we have a 4.9/5.0 average appointment rating, and 85% of users rate the support they received from Maven as “very good” or “excellent.” This keeps users coming back and enables interventions that drive outcomes (the holy grail in healthcare).
In addition to driving best-in-class product utilization, our customer-centric formula also leads us to new insights and new approaches that our clients may not be asking for, but that ultimately benefit them. For instance, we recently launched Maven Wallet, a reimbursement product, because our members were struggling with fertility and adoption reimbursement — frustrating members and leading to lost time at work or with their families. We launched Maven Milk, a breastmilk shipping product, in 2018, because we consistently observed breastfeeding schedules as a blocker to successful returns to work. And in 2017, we instituted manager training as an integral part of our return-to-work experience, because we saw manager/company culture as a significant trigger prompting new moms to drop out of the workforce.
* * *
Maven is only six years old, and we are still in the early stages of learning — so I won’t be so bold to assert that the formula above is the final word, or is fully exhaustive. It’s simply our point of view, based on the evidence we’ve gathered to date, on what types of interventions will drive the real value that clients/payors so desperately seek, and ultimately what will create healthier outcomes for women and families.
The core theme, which I personally find exciting, is one of a model that understands women’s and family health not as a vertical, but as the very core of a functional healthcare system. The advent of a family is a point of provenance — for a newborn baby, obviously, but also for engagement with a new range of healthcare providers, and ultimately for future health outcomes. Getting this right — for women, families, children — promotes positive outcomes throughout life, and system-wide.
For us at Maven, having the opportunity to tackle these entrenched, systemic issues has been humbling, exciting, maddening, and deeply rewarding. And for me, as a mother of two, it’s also deeply personal. We feel good about what we’ve done, and we’re excited for where we’re going.
Ready to get started with Maven?
See how Maven can support working families, retain talent, and reduce costs








.jpeg)